Quality Awards Summary
About the Award
Established in 2021, the NAACOS Leaders in Quality Excellence Awards recognize ACOs working to improve the quality and safety of patient care and advance population health goals. Following an open call for nominations, the NAACOS Quality Committee selected the top three to showcase quality improvement efforts undertaken by NAACOS members and to disseminate best practices. The three 2022 winners—Delaware Valley ACO, UT Southwestern ACO, and University of California San Francisco Health—exemplify how ACOs across the country are improving care, demonstrate how ACOs are closing gaps in care, improving care coordination for complex patients, and addressing disparities in care. The following criteria were used to select the winners:
- Innovation—in processes or technology used to improve performance.
- Improvement—in quality as a result of the intervention or innovative strategies used.
- Scalability and long-term contributions—how can the project’s work be continued, is it scalable, sustainable, transferrable and what was the return on investment.
Delaware Valley ACO Invests in Home-Based Palliative Care
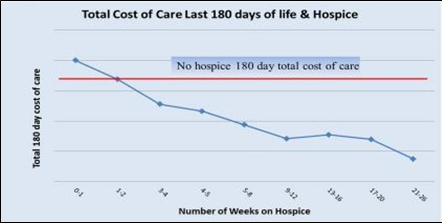
To improve care for patients and families facing serious illness or nearing the end of life, the Delaware Valley ACO created a home-based palliative care strategy. A team of clinicians and analysts built clinically relevant claims-based views of end-of-life care among the ACO’s Medicare patients and national benchmarks. They found almost half of the ACO’s patients (47%) received hospice care for a week or less before death, much higher than the 28% nationally. Further analysis showed that longer hospice stays helped reduce the total cost of care.
The ACO used the findings to build the case for earlier activation of palliative care, which centers on pain and other symptom management, care coordination and planning, and assessment and support of caregiver needs. Advance care planning toolkits were distributed to clinicians with tailored information and resources. Services included in-home provider visits and access to

social work and chaplain services, rehabilitation therapy, 24/7 on-call help with in-home visit capabilities, telehealth, telemonitoring, and advanced illness management services.
The share of patients receiving hospice for one week or less before death improved from 47% to 32%. Along with providing more positive end-of-life experiences for patients and families, an analysis found that patients receiving home-based palliative care resulted in savings of about $9,000 in the last 90 days of life compared to patients who didn’t receive palliative care. Moreover, providing home-based palliative care to patients before death reduced emergency department visits by 35%, inpatient admissions by 51%, and inpatient length of stay by 1.5 days. The program also increased the percentage of the ACO’s seriously ill population with an advance care plan from 25% to 46%.
Using Artificial Intelligence to Pinpoint Patients at High Risk of Unplanned Hospitalizations
UT Southwestern ACO, also known as Southwestern Health Resources, developed a novel risk stratification algorithm using artificial intelligence machine learning techniques to match high-risk patients with complex care management services to prevent potentially avoidable hospitalizations and Emergency Department visits. Leveraging data from claims and electronic health records, the ACO built predictive models and integrated and trained the models with data from publicly available social determinants of health data sets, such as the Social Vulnerability Index and the Area Depravation Index, to identify socioeconomic barriers to care at the individual level. The ACO then encouraged patients to enroll in a longitudinal complex care management program.

Using personalized care management plans, patients received tailored support and care coordination for clinical, social, pharmaceutical, and behavioral health needs. The
high-intensity multidisciplinary care management program spans 3-4 months and then community health workers follow patients for an additional two months, checking in with patients at least every two weeks and escalating issues to the larger, multidisciplinary team if needed.
An analysis six months after the intervention found two unplanned hospital admissions among the 25 patients who received complex care management, compared to 31 unplanned hospital admissions among 91 patients who did not receive enhanced care management. The ACO plans to scale the intervention, setting a goal to engage 1,800 patients by the end of 2023. An anticipated success rate of 80% would avoid 1,440 unplanned hospital admissions, which at an estimated average cost of $15,000 per admission would equate to $22 million in cost avoidance.
Using Artificial Intelligence to Pinpoint Patients at High Risk of Unplanned Hospitalizations

After identifying a 10-point gap in 2020 between Black (67.6%) and White patients (77.8%) with controlled high blood pressure, University of California San Francisco Health set a health equity goal of reducing hypertension disparities.
As the impact of the COVID-19 pandemic grew, the ACO found the percentage of patients with controlled blood pressure declined significantly. Similarly, patients were less likely to receive in-person care, so many lacked a recent blood pressure reading. Working with UCSF health disparities researchers, the ACO conducted interviews with Black patients to better understand their preferences, barriers, and competing priorities. Based on patient input, the ACO designed interventions, including culturally tailored hypertension educational materials. The ACO also developed a team-based coordinated intervention among primary care, pharmacy, and
population health to help patients manage their hypertension. Patients with uncontrolled hypertension were offered a 2- to 3-month

intensive program with telehealth pharmacist visits to review medication management and coaching from health care navigators to support smoking cessation and other healthy behaviors associated with controlling hypertension.
The ACO launched a separate effort for patients with hypertension and no recent blood pressure reading. Health navigators mailed home blood pressure monitors, taught patients to use them via the phone and video conferencing, and collected remote blood pressure readings. Patients with out-of-range readings were scheduled for primary care appointments. In-clinic distribution of blood pressure cuffs and nursing-based patient education were also used. A year after implementation, disparities in blood pressure control narrowed significantly, with 73.1% of Black patients attaining blood pressure control compared with 74.3% of the overall population.