NAACOS Analysis of the Proposed 2021 Medicare Physician Fee Schedule
Executive Summary
In early August, the Centers for Medicare & Medicaid Services (CMS) released the proposed 2021 Medicare Physician Fee Schedule (MPFS) rule. This proposed regulation includes a number of policies affecting Medicare physician payment, quality measure changes for Medicare Shared Savings Program (MSSP) ACOs, and Quality Payment Program (QPP) requirements for 2021. The key proposals affecting ACOs are outlined below and further detailed in this analysis. The rules are summarized in this CMS factsheet along with detailed QPP changes. In addition to this document, NAACOS also hosted a webinar on the proposed rule, which can be viewed on-demand.
NAACOS is seeking member input on the proposals in this rule, which will help shape our comments. Please share your feedback by emailing us at [email protected]. CMS will review comments and issue a final rule later this year. Typically, the final MPFS rule is released around November 1, but CMS notes that due to prioritization of efforts related to the COVID-19 pandemic, the agency may issue the final rule later this year.
Medicare Shared Savings Program Proposals
Medicare Physician Payment Proposals
Quality Payment Program (QPP) Proposals
MEDICARE SHARED SAVINGS PROGRAM
MSSP Quality Changes
CMS proposes major structural changes to the way MSSP ACOs are measured and assessed on quality. For 2021 and future performance years, CMS proposes to sunset the current approach of quality measurement for MSSP ACOs and replace it with a new APM Performance Pathway (APP) to better align with the Quality Payment Program (QPP). CMS also notes many ACOs are currently high performers under the current structure and the agency believes it is appropriate to require a higher standard of care in order for ACOs to continue to share in any savings they achieve. CMS also notes they believe holding ACOs to a higher standard is in line with CMS goals of incentivizing value-based care and driving the Medicare system to greater value and quality.
Notably, the new APP would include fewer measures and a higher minimum attainment standard, which is the threshold that ACOs would be evaluated on to be eligible to share in savings earned.
Proposed APP Measure Set
CMS proposes to dramatically decrease the number of measures ACOs are evaluated on for purposes of MSSP quality assessments. Table 36 on page 50233 of the proposed rule outlines the proposed new measure set for MSSP ACOs.
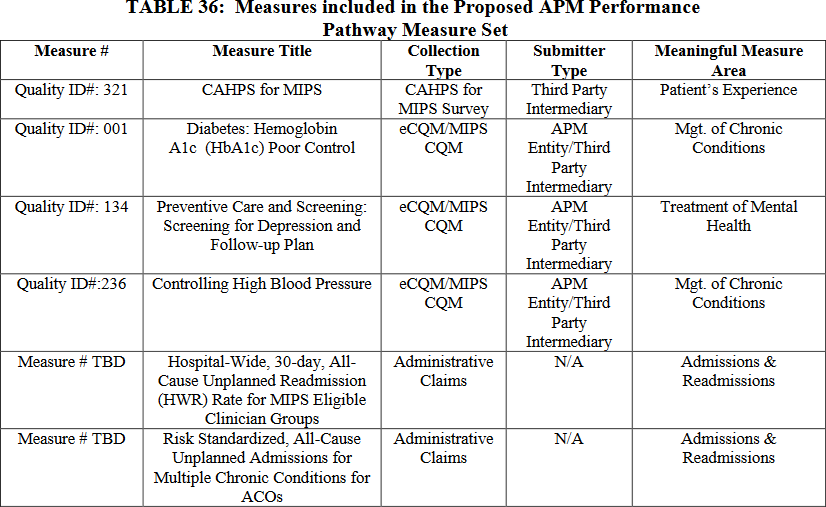
Note that CMS counts each Consumer Assessment of Healthcare Providers and Systems (CAHPS) for ACOs survey measure as an individual measure under the current program structure (totaling 10 measures), while this proposed APP measure set would count all CAHPS for MIPS survey measures as one measure. The proposed new measure set would include three clinical quality measures, the CAHPS for MIPS survey measures (counted as one measure), and two administrative claims measures. Note the readmission measure is specified for MIPS and is therefore slightly different from the readmission measure currently used to assess ACOs. Finally, CMS notes the agency will propose a new, “Days at Home” measure that is currently under development, in future years.
Reporting Mechanisms
CMS propose to eliminate the Web Interface as a reporting method for ACOs and all MIPS reporters beginning in 2021, citing low uptake of use outside the ACO program. In place of the Web Interface, the APP would require ACOs to actively report on three clinical quality measures (see table 36 above), which could be reported using a registry or direct via electronic health records (EHRs) using electronic clinical quality measure (eCQM) standards. Note that eCQMs must be reported for all patients, regardless of payer. This is a very significant change, and ACOs should consider the operational changes that may be necessary to make these adjustments.
Scoring Methodology
CMS proposes to alter the scoring methodology currently used to assess MSSP ACO quality. Currently, ACOs are scored within four equally weighted domains. An ACO earns quality points for each measure on a sliding scale based on level of performance. For measures that are pay-for-reporting, ACOs receive full points if the ACO completely and accurately reports for that measure. These points roll up to the maximum points allowed for each domain. CMS also provides up to four points per domain for significant improvement. CMS calculates a percent score for each domain (i.e., the sum of points earned and improvement points divided by the total available quality points for that domain). ACOs receive an overall quality score (sum of all domain percent scores divided by four domains). See CMS website (refer to quality measurement section) for sliding scale and points available per domain. NAACOS also has developed a Quality Reporting guide with more information on the current scoring approach (refer to scoring chapter). Finally, the current minimum attainment standard requires ACOs to meet or exceed the 30th percentile among all Web Interface reporters on at least one measure in each of the four quality domains.
As proposed, CMS would instead award a score of three-to-ten points for each measure in the APP that meets the data completeness and case minimum requirements, which would be determined by comparing measure performance to established benchmarks. Note that benchmarks would no longer be determined by looking at all Web Interface reporters, but rather, benchmarks would be established based on all MIPS reporters. Benchmarks will also vary based on the reporting method chosen by the ACO. Notably, CMS is proposing to remove the pay-for-reporting year currently provided to ACOs in their first year. CMS also proposes to change the minimum attainment standard to require ACOs to meet or exceed the 40th percentile among all MIPS reporters. Finally, as is currently the case, ACOs must also report on all measures in order to meet the minimum attainment standard. CMS clarified in an email to NAACOS staff in September that ACOs final score on all six measures will be evaluated against the minimum attainment standard of the proposed 40th percentile.
Finally, note that CMS is also proposing to adjust the current MIPS quality measure benchmarking rules due to data anomalies presented by COVID-19. Specifically, CMS proposes to use CY 2021 data to determine PY 2021 quality benchmarks. Should CMS finalize these proposals, this will result in ACOs not knowing quality benchmarks in advance of the performance year. CMS seeks comment on alternative approaches.
Quality Scores and Shared Savings/Loss Rates
Currently, ACOs must meet minimum attainment standard to be eligible to share in any savings earned by the ACO. Once the minimum attainment standard is met, the quality score determines an ACO’s shared savings or loss rate. The better the score the more savings earned; the better the score the less an ACO must repay.
CMS proposes that instead ACOs must meet the minimum attainment standard to be eligible to share in any savings earned, however, once the minimum standard is met an ACO would receive the maximum shared savings rate automatically regardless of the ACO’s final quality score. If an ACO does not meet the minimum attainment standard, the ACO would not be eligible for shared savings. To determine shared loss rates, CMS proposes to use an approach that would award ACOs with higher quality scores a lower shared loss rate (and vice versa), except for risk-based Basic Track ACOs that will continue to apply a fixed 30 percent shared loss rate. Finally, CMS notes ACOs that fail to meet the minimum attainment standard and are responsible for shared losses would owe the maximum shared loss rate.
Alternative Proposal Allowing ACO Selection of Quality Measures
CMS also seeks comment on an alternative approach that ACOs could use in the event “the three measures ACOs are required to actively report on are not applicable to their beneficiary population.” In this case, the ACO could choose to opt out of the APP and report to MIPS as an APM Entity selecting more appropriate measures available under MIPS. CMS does not include any further details regarding how CMS would determine if the three required measures were not applicable to the ACO.
Quality Compliance
CMS proposes to strengthen policies for compliance with the quality performance standard by broadening the conditions for which CMS may terminate an ACO’s participation agreement. Specifically, CMS proposes to terminate an ACO’s participation agreement when the ACO fails to meet the quality performance standard for two consecutive performance years within an agreement period or fails to meet the quality performance standard for any three performance years within an agreement period, regardless of whether the years are consecutive. Finally, CMS proposes to change the Data Validation and Audit process to align with MIPS.
Quality and the ACO Extreme and Uncontrollable Circumstances Policy
CMS proposes to make changes to the quality portion of the Extreme and Uncontrollable Circumstances policy for ACOs to align with the proposed changes to introduce a new APP for ACOs. For PY 2021 and subsequent years, CMS proposes to provide an ACO affected by an extreme and uncontrollable circumstance with the higher of its own quality score or a score equal to the 40th percentile MIPS Quality performance category score. CMS also proposes to use the quarter four list of assigned beneficiaries to determine the portion of patients affected by the extreme and uncontrollable circumstance.
In addition, CMS seeks comment on a potential alternative Extreme and Uncontrollable Circumstances Policy for PY 2022 and subsequent years. Specifically, CMS proposes to adjust the amount of shared savings determined for affected ACOs that complete quality reporting but do not meet the quality performance standard, or that are unable to complete quality reporting. Under this alternative approach, CMS would determine shared savings for an affected ACO by multiplying the maximum possible shared savings the ACO would be eligible to receive based on its financial performance and track (or payment model within a track) by the percentage of the total months in the performance year affected by an extreme and uncontrollable circumstance and the percentage of the ACO’s assigned beneficiaries who reside in an area affected by an extreme and uncontrollable circumstance.
Modifications to 2020 Quality Reporting Requirements and the Extreme and Uncontrollable Circumstances Policy Due to COVID-19
Due to the negative impacts of COVID-19 on sample size and performance scores, CMS proposes to remove the requirement for ACOs to field a CAHPS for ACOs survey for PY 2020. Instead, CMS proposes to provide automatic full points for each of the CAHPS survey measures within the patient/caregiver experience domain for PY 2020. Additionally, CMS seeks comment on, but does not formally propose, to alter the 2020 Extreme and Uncontrollable Circumstances Policy for ACOs to award ACOs the higher of their 2019 or 2020 quality scores, so long as the ACO fully reports quality in PY 2020. NAACOS has advocated since March for CMS to make accommodations to quality reporting requirements for 2020 given the COVID-19 pandemic, and we are very pleased to see CMS propose these important changes.
MSSP Beneficiary Assignment
CMS proposes to amend the list of primary care services it uses to assign beneficiaries to ACOs by adding nine more codes and making technical changes to existing codes used in assignment starting in PY 2021. The additional proposed codes include:
*not yet finalized
The proposed additions are similar to codes currently used in beneficiary assignment, CMS states, therefore, making it logical to add these nine services. The principal care management and non-complex chronic care management codes were added to the fee schedule last year. E-visits, which were added in 2019, are non-face-to-face, patient-initiated communications using online patient portals with established patients. Elsewhere in this regulation, CMS is proposing to add GCOL1, which would pay for 30 minutes of behavioral health manager time in the Psychiatric Collaborative Care Model.
Earlier this year in rulemaking related to the COVID-19 PHE, CMS added G2010 (remote evaluation of patient video/images), G2012 (virtual check-ins), 99421-99423 (e-visits), and 99441-99443 (newly covered telephone E/M services) to the list of codes used in patient attribution for ACOs for PY 2020 and any subsequent performance year that starts during the COVID-19 PHE. CMS is seeking comment on whether to permanently add G2010 and G2012 to the ACO assignment list.
CMS also proposes to exclude advance care planning (99497 and 99498) when billed in an inpatient setting from being used to determine beneficiary assignment starting in PY 2021. CMS states it believes not placing any exceptions of the place of service or provider type may result in patients being assigned to ACOs because of inpatient care rather than primary care services by their regular health provider. CMS found that more than 13 percent of the 1.6 million claims in 2019 for advance care planning took place in an inpatient setting. If finalized, CMS will adjust ACOs’ historical benchmarks to account for any changes to ACO beneficiary assignment it makes.
CMS also proposes to exclude professional services furnished by Federally Qualified Health Centers (FQHCs) or Rural Health Centers (RHCs) when those services are delivered in a SNF. In the 2019 MPFS, CMS finalized a policy to exclude CPT codes 99304 through 99318 when delivered in a SNF, effective starting in 2019. CMS would identify such services by the presence of a SNF facility claim with dates of services that overlap with the date of the professional service. Previously, CMS excluded claims with a place of service code 31, signifying the service was delivered in a SNF. However, because FQHC and RHC claims are submitted using institutional claim forms, CMS doesn’t exclude CPT codes 99304 through 99318 from ACO assignment when provided in a SNF. If finalized, CMS will adjust ACOs’ historical benchmarks to account for any changes to ACO beneficiary assignment it makes.
MSSP Repayment Mechanism Requirements
To correct unintended consequences and burdens associated with the repayment mechanism requirements, CMS proposes certain policy changes. Currently, a renewing ACO that wants to use its existing repayment mechanism in the subsequent agreement period is required to maintain a higher repayment mechanism amount than necessary for its new agreement period if the repayment mechanism amount for the last performance year of the previous agreement period is greater than what is needed for the subsequent agreement period. CMS proposes to eliminate this requirement.
Under the Pathways to Success regulations, summarized in this NAACOS resource, when a recalculated repayment mechanism increases by a certain amount (i.e., the lesser of 50 percent or $1,000,000), CMS requires the ACO to increase the value of the repayment mechanism. However, CMS does not decrease the repayment mechanism amount when the opposite occurs, a policy for which NAACOS has advocated. In this rule, the agency proposes to allow ACOs an option to decrease their repayment mechanism amounts if the recalculated amount is less than the current amount. If finalized, this policy would be in place beginning with PY 2022. The agency also proposes to allow eligible ACOs that renewed their agreements effective July 1, 2019, or January 1, 2020, a one-time opportunity for a repayment mechanism decrease. If finalized, the agency would notify eligible ACOs of their opportunity to reduce repayment mechanism amounts after the start of PY 2021.
Track 1+
CMS clarifies that to align Track 1+ policies with MSSP policies, the agency is providing Track 1+ ACOs whose agreement periods are set to expire December 31, 2020 an opportunity to voluntarily extend their agreement period for a fourth performance year in 2021. Additionally, CMS clarifies that the proposed MSSP policies in this rule would apply to Track 1+ ACOs in the same way they apply to Track 1 ACOs as long as the applicable regulation has not been waived under the Track 1+ Model. Therefore, policies detailed above such as changes to MSSP quality and assignment would apply to Track 1+ ACOs, if finalized. A specific list is available on page 50251.
PHYSICIAN PAYMENT AND POLICY CHANGES
Overview
As is typical in the MPFS, CMS outlines proposed 2021 relative value units (RVUs), which include work, malpractice, and practice expense (PE) RVU updates. These building blocks of the MPFS are adjusted over time to reflect new developments and services as well as shifts in payments within the fee schedule. The agency also identifies payment changes through its process to update what it determines are misvalued services. Geographic Practice Cost Indices (GPCIs) are another essential component of MPFS payments and, following a scheduled three-year update in 2020, CMS does not propose notable GPCI updates for 2021.
With the budget neutrality adjustment to account for changes in RVUs, as required by law, the estimated Calendar Year (CY) 2021 MPFS conversion factor is $32.26, a notable decrease from the CY 2020 MPFS conversion factor of $36.09. This decrease is in part due to a 0 percent automatic conversion factor update from the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and reflects the overall payment increases for outpatient/office Evaluation and Management (E/M) services, which lead to payment decreases in other areas of the MPFS to maintain budget neutrality. More detail on specific payment changes and shifts among specialties can be found in the following:
Care Management Services
As part of evaluating payment for Medicare services, the CMS considers updates to care management services which many ACOs use as part of their overall care coordination strategy. Table 13 on page 50117 provides a summary of care management codes. For 2021, CMS proposes to update billing policies for Transitional Care Management (TCM) codes 99495 and 99496. Specifically, the agency proposes to remove 15 codes from the list of codes that may not be billed concurrently with TCM. Those codes are shown in table 14 on page 50120. Under another care management proposal related to expanding use of Psychiatric Collaborative Care Model services, CMS proposes to establish a G-code, GCOL1, to describe 30 minutes of behavioral health care manager time. Finally, CMS proposes to add Principal Care Management Services, HCPCS codes G2064 and G2065, to the existing comprehensive care management service for Rural Health Clinics and Federally Qualified Health Centers, G0511, starting January 1, 2021, which will be added to the calculation of the G0511 payment rate.
Evaluation and Management Services (E/M)
In total, E/M visits comprise approximately 40 percent of allowed charges for PFS services; and office/outpatient E/M visits, in particular, comprise approximately 20 percent of allowed charges for PFS services. CMS has long acknowledged the need to revise payment, guidelines, and documentation requirements for billing E/M services and has taken notable steps in recent years to do so. In the final 2020 MPFS rule, summarized in this NAACOS resource, the agency finalized significant changes to outpatient and office E/M services, including implementing a revised approach to updating E/M services based on a framework from an American Medical Association Current Procedural Terminology (AMA CPT) Workgroup on E/M. The proposed 2021 MPFS rule continues the approach finalized in last year’s rule.
To maintain relativity with the increased office/outpatient E/M values, CMS proposes to revalue certain services and code sets that include, rely upon, or are analogous to office/outpatient E/M visits. Among the codes and codes sets with values closely tied to the those for office/outpatient E/M visit codes are: TCM services (CPT codes 99495, 99496); cognitive impairment assessment and care planning (CPT code 99483); certain end-stage renal disease (ESRD) services (CPT codes 90951 through 90970); and the annual wellness visit (AWV) and initial preventive physical exam (IPPE) (HCPCS codes G0402, G0438, G0439), among others. Many of these services were valued via a building block methodology and have office/outpatient E/M visits explicitly built into their definition or valuation. CMS proposes to update the valuation of these codes, including RVU and input changes shown in Table 19 (page 50128) and Table 20 (page 50132).
CMS also proposes to adjust a code that the agency finalized last year which will go into effect in 2021. This add-on code, 99XXX, is for prolonged office or other outpatient E/M services, requiring total time beyond the usual service, and reflects additional resources used for E/M codes 99205 and 99215. CMS proposes that when the time of the reporting physician or non-physician practitioner (NPP) is used to select office/outpatient E/M visit level, CPT code 99XXX could be reported when the maximum time for the level 5 office/outpatient E/M visit is exceeded by at least 15 minutes on the date of service.
There is wide variation in the volume and level of E/M visits billed by different specialties. According to Medicare claims data, E/M visits are furnished by nearly all specialties but represent a greater share of total allowed charges for physicians and other practitioners who do not routinely furnish procedural interventions or diagnostic tests. Generally, these practitioners include primary care practitioners and certain other specialists such as neurologists, endocrinologists and rheumatologists. Therefore, the combined effect of E/M payment revisions along with valuation changes for codes related to E/M, results in more considerable payment shifts among different providers within the MPFS than what has been typical in the last few years. These payment shifts can be seen in Table 90 on page 50375.
Telehealth and Other Services Involving Communications Technology
Additions to the Medicare Telehealth List
CMS proposes to permanently add nine codes to the list of those eligible to be delivered via telehealth. CMS proposes to temporarily add another 13 codes on the Medicare telehealth list through the calendar year for which the COVID-19 PHE ends so that more evidence can be collected on their use. In an interim final rule published in the Federal Register on April 6, CMS temporarily added about 80 codes to the Medicare telehealth list during the COVID-19 PHE. In this proposed rule, CMS states that it reviewed those temporary additions to see if they met the agency’s criteria to be added permanently to the telehealth list. Services must have a demonstrated clinical value when delivered via telehealth to be added to the permanent list.
However, there are 60 other codes that were added to the Medicare telehealth list during the PHE for which CMS is declining to permanently add to the eligible list. These include ESRD treatment, psychological and neuropsychological testing, physical and occupational therapy, observational stay care for hospitals, intensive care units (ICUs), and emergency care, higher level emergency department (ED) visits, observation and discharge day management visits, critical care visits, and others. A full list of codes is included on Table 12 of the proposed rule, which is copied below.
CMS singles out three sets of services — initial and final/discharge interactions (CPT codes 99234–99236 and 99238–99239), higher-level emergency department visits (CPT codes 99284–99285), and hospital, ICU, emergency care, observation stays (CPT codes CPT 99217–99220; 99221–99226; 99484–99485, 99468–99472, 99475–99476, and 99477–99480) — for specific feedback on. These services, CMS says, could have potential benefit if delivered via telehealth but need some sort of in-person interaction to be fully delivered. CMS also seeks comment on other codes that could be delivered via telehealth in certain circumstances, for example in some models of care delivery that utilize a combination of remote monitoring and clinical staff at the location of the beneficiary to allow, when an onsite supervising practitioner is not available, for a supervising practitioner at a distant site to monitor vital signs and direct in-person care as needed.
Summary of CY 2021 Proposals for Addition of Services to the Medicare Telehealth Services List
Type of Service
Specific Services and CPT Codes
Services CMS is proposing for permanent addition to the Medicare telehealth services list
Services CMS is proposing to temporarily add to the Medicare telehealth services list
Services CMS is not proposing to add to the Medicare telehealth services list but is seeking comment on whether they should be added on either a temporary or permanent basis.
While two-sided risk ACOs who use prospective assignment have an exception through the MSSP telehealth waiver, CMS notes that patients’ homes are not generally a permissible telehealth originating site. An exception, however, was added by the SUPPORT Act of 2018, which made telehealth allowable in patients’ homes for the purposes of treating substance use disorder or a co-occurring mental health disorder to an individual with a substance use disorder diagnosis. Therefore unless provided to prospectively assigned patients in a two-sided ACO model, the domiciliary/home visits codes either permanently or temporarily added to the Medicare telehealth list could be billed via telehealth for services to treat substance use disorder or cooccurring mental health disorder.
Comment Solicitation on Continuation of Payment for Audio-only Visits
Federal law generally defines telehealth as a live, interactive audio-video visit. During the COVID-19 PHE, CMS moved to allow certain services to be delivered through audio-only technology, such as simple phone calls. The agency also established payment for three telephone E/M services (99441–99443) that were previously not covered, increasing their reimbursement under a May 1 interim final rule to be cross-walked with 99212–99214. A more complete rundown of CMS’s allowances during the PHE can be found in this NAACOS resource.
CMS states in the proposed rule that it doesn’t intend on paying for these audio-only services after the PHE ends. However, the agency recognizes that phone-based visits are important to continue after the PHE as beneficiaries may still lack access to the technology that live, video-based visits usually require. Therefore, CMS seeks comment on creating new codes and payment for audio-only visits. These new codes may parallel Medicare’s “virtual check-ins” (G2012), which are brief, 5-to-10 minute telephone calls with patients that aren’t related to medical visits in the last seven days and don’t lead to a medical visit in the next 24 hours. The agency also seeks comment on additional non-face-to-face services that could be delivered through technology, but that Medicare doesn’t currently cover. Additionally, CMS wants to know any impediments or barriers providers face to bill for telehealth, remote patient monitoring, or other communications technology-based services.
Creation of More Communication Technology-Based Services
CMS proposes to establish two new codes that can be billed by non-physician practitioners and others who cannot independently bill for E/M services. G20X0 and G20X2 cover the remote assessment of recorded video and/or images submitted by established patients and brief, 5-to-10 minute telephone calls with established patients. These codes are analogous to Medicare’s “virtual check-in” codes created in the 2019 fee schedule, but those 2019 codes are only billable by practitioners who can furnish E/M services.
Furnishing Telehealth Visits in Nursing Facility Settings
CMS seeks comment on Medicare allowing initial skilled nursing facility (SNF) visits from physicians and other clinicians to be via telehealth. CMS requires these visits and certain subsequent visits to be in-person, but the agency waived those in-person requirements during the COVID-19 PHE. CMS also proposes to allow subsequent nursing facility visits to be conducted via telehealth once every three days, rather than the current 30-day limit. CMS also seeks feedback on the necessity of CMS’s frequency limitations more broadly and how often services can be conducted through telehealth.
Changes to Supervision Requirements Through Telehealth
During the PHE, CMS has allowed direct supervision to include the virtual presence of a supervising physician or clinician using interactive, real-time audio-video technology. CMS proposes to extend this policy through at least 2021 or the year in which the PHE ends to give the agency more time to solicit feedback and make additional changes as needed. Additional “guardrails” or limitations may be needed to ensure patient safety and clinical appropriateness.
CMS makes a number of other clarifications to policies that have arisen during the PHE. Services that may be billed “incident-to” may be provided via telehealth under direct supervision of the billing professional. If a telehealth visit is provided when the patient and physician are in the same institutional or office setting, then the service should be billed as if it were in-person.
Clarification of Allowable Telehealth Technology
Lastly, CMS proposes to remove from the regulatory definition of allowable technology “[t]elephones, facsimile machines, and electronic mail systems that do not meet the definition of an interactive telecommunications system” to eliminate confusion whether smartphones may be permissible technology.
Remote Physiologic Monitoring Services
In recent years, CMS has moved to greatly expand payment of services for the remote monitoring of patients’ physiologic condition. Seven codes now exist that cover remote patient monitoring (RPM). Also, during the COVID-19 PHE, CMS has created several policies that seek to increase use of RPM during the pandemic in an effort to reduce in-person office visits.
In this proposed rule, CMS clarified that it will allow patient consent to be obtained at the time RPM services are delivered. Additionally, RPM may be billed to patients with acute conditions, as well as chronic conditions. However, once the COVID-19 PHE ends, CMS will restrict RPM services to established patients and once again require that data be collected for 16 days within a 30-day period to bill for 99453 and 99454, which pay for RPM set-up, patient education and monitoring. Furthermore, those codes may only be billed once per patient per 30-day period and only when at least 16 days have been collected, even when multiple devices can be billed. However, auxiliary personnel, including contracted employees, may furnish CPT codes 99453 and 99454 services under a physician’s supervision. In order for 99454 to be billed, CMS clarifies that a medical device used for RPM must be one approved by the Food and Drug Administration and must automatically upload patient data — that is not rely on patient self-recorded and/or self-reported data.
For CPT codes 99457 and 99458, which pays for “interactive communication” between a clinician and a patient or caregiver, CMS clarified that the device must involve, at a minimum, a real-time synchronous, two-way audio interaction that is capable of being enhanced with video or other kinds of data transmission.
CMS, however, is seeking comment on whether the current suite of RPM billing codes accurately and adequately describes the full range of clinical scenarios that may benefit patients. For example, CMS requires 16 days or more of data every 30 days for codes to be billed. But patients, especially those with acute illnesses that CMS clarified are eligible for RPM, may benefit from fewer than 16 days of remote monitoring. The agency is considering new billing codes and payment rules that would allow clinicians to bill and be paid for RPM with shorter monitoring periods.
QUALITY PAYMENT PROGRAM (QPP)
Advanced APMs
Predicted Number of Qualifying APM Participants (QPs)
As required under MACRA, QP thresholds rise over time, making it more challenging to earn the Advanced APM bonus. In PY 2021, which corresponds to Payment Year 2023, the QP payment amount threshold increases from 50 percent to 75 percent, and the QP patient count threshold increases from 35 percent to 50 percent. Despite a growing number of Advanced APMs, CMS predicts that the number of QPs will go down slightly in PY 2021 as compared to 2019 and 2020. Specifically, the agency estimates that there will be between 196,000 and 252,000 QPs for PY 2021 with total bonuses of between $700 million and $900 million. NAACOS has repeatedly advocated to modify QP calculations, and we have worked with our congressional champions to introduce the Value in Health Care Act, summarized here, which would prevent the QP thresholds from rising in 2021.
Advanced APM Incentive Payment
CMS proposes to clarify that the Advanced APM incentive amount is calculated based on the paid amount, not the allowed amount, of the applicable claims for covered professional services that are aggregated to calculate the estimated payments. This clarification comes after NAACOS pointed out previous CMS regulations and language indicating that the agency initially indicated the bonus would be based on the allowed amount. NAACOS has advocated that the agency’s implementation reflect its initial language, and we are disappointed to see this clarification.
CMS acknowledges the complexity of distributing Advanced APM bonuses when clinicians are no longer practicing at TINs associated with earning their Advanced APM bonus. Therefore, the agency proposes an eight-step hierarchy for identifying where to pay the Advanced APM bonus, starting with a Tax Identification Number (TIN) tied to where the QP earned the Advanced APM status and ending with a proposal to publicly list QPs for whom the agency could not identify a TIN to which to make the payment and requiring those QPs to contact CMS and provide Medicare payment information.
QPs and Partial QP Determinations
Currently, for QP calculations, a beneficiary may be counted only once in the numerator and denominator for a particular ACO (or APM Entity) but that a beneficiary may be counted multiple times across the numerators and denominators for different ACOs (or other APM Entities). In this rule, CMS acknowledges that when a beneficiary is prospectively assigned to an ACO or other APM Entity, and therefore could not possibly be assigned to other ACOs or APM Entities, it is unfair to include that beneficiary in those QP calculations. Therefore, CMS proposes to exclude prospectively assigned beneficiaries from the denominators of other ACO/APM Entity QP calculations when that beneficiary is ineligible to be added to the ACO/APM Entity’s list of assigned beneficiaries. Effectively, this decreases the QP denominator, thus increasing the overall QP score.
Partial QP Election and Targeted Review
In an attempt to ease administrative burdens, CMS requests comment on whether to allow an APM Entity, such as an ACO, to make the Partial QP election on behalf of all of the individual eligible clinicians associated with the APM Entity. The election would apply to whether the Partial QPs want to participate in MIPS and have MIPS payment adjustments since Partial QPs are ineligible to earn Advanced APM bonuses as a result of falling short of QP thresholds.
CMS proposes to establish a targeted review process for limited circumstances surrounding QP determinations, such as to review CMS clerical errors like omitting a clinician from a Participation List used for QP determinations. After a specified time period for a targeted review, there would be no further review of QP determinations with respect to an eligible clinician for the QP Performance Period, and there continues to be no administrative or judicial review for QP determinations. If CMS determines a clinician was missing due to CMS clerical error, the agency proposes to assign the ACO or APM Entity’s most favorable QP score from that performance year. A review could be submitted by an eligible clinician or APM Entity during a specified 60-day review period announced by CMS.
MIPS Proposals
CMS proposes very minor updates to MIPS for 2021. Notably, CMS proposes to not move forward with the MIPS Value Pathways (MVP) approach for 2021 due to the strains placed on the health care system related to the COVID-19 pandemic. Instead the agency continues to solicit feedback on the guiding principles for implementing the MVP in 2022 at the earliest.
CMS proposes to sunset the MIPS APM Scoring Standard, the scoring method currently used for ACOs in MIPS, starting in 2021. Instead CMS propose to replace the MIPS APM Scoring Standard with the new APM Performance Pathway (APP) that will also be used to score MSSP ACOs quality for purposes of the MSSP.
ACO Scoring in MIPS under the APP
CMS proposes to score ACOs subject to MIPS using the APP framework. This framework is similar to, but not the same as the current MIPS APM Scoring Standard. Note the APP will be used for all MIPS APMs that select this option. For MSSP ACOs, reporting under the APP is required for purposes of the MSSP quality assessments, and that information will also be used for scoring quality in MIPS.
Overview of Proposed Changes for ACOs Under the APP for MIPS Assessments
Performance Category
Proposed Weights
Notable Changes Proposed
Quality
50%
Moves to APP structure and measure set as well as scoring approach.
Cost
0%
No changes proposed for ACOs. ACOs would continue to not be given a Cost score in MIPS.
Improvement Activities
20%
No changes proposed for ACOs. ACOs would continue to be awarded full points automatically for improvement activities.
Promoting Interoperability
30%
No changes proposed for ACOs. All individual and group scores would continue to be averaged, using a weighted average based on the number of clinicians in a group, to determine one average ACO Promoting Interoperability score.
A very notable difference in this proposed approach would allow individual clinicians and groups TINs the option of choosing to report outside the ACO for purposes of MIPS analysis. Should a practice or clinician choose this option, it would be required to select the appropriate measures and reporting method and report separately from the ACO for purposes of MIPS scoring. In this case, these clinicians/groups would only be provided with 50 percent automatic credit for improvement activities (while ACOs are awarded with full points automatically for this performance category). CMS would then award the clinician with the higher of their own score or the ACO’s score for MIPS.
Another key proposed change is regarding how CMS will award a MIPS score when a clinician has multiple final scores associated with a single TIN/NPI combination. CMS proposes to use the following hierarchy to assign a final score in these instances:
- Virtual Group final score
- Highest available score from an APM Entity (such as an ACO), group and/or individual clinician
Currently, CMS uses the following hierarchy:
- APM Entity score (highest score if multiple exist)
- Virtual Group final score
- Group or individual clinician score (whichever is higher)
Finally, CMS notes they propose the MIPS quality measure scoring cap for topped out measures will not apply to clinicians, groups or APM Entities (such as an ACO) reporting through the APP. Instead should an APP measure be determined to be topped out, CMS will amend the measure set as appropriate through rulemaking.
APM Entity Groups in MIPS
CMS proposes to end the full-TIN APM requirement given the removal of the APM Scoring Standard. Given this, CMS proposes that MIPS eligible clinicians identified on the Participation List or Affiliated Practitioner List of any APM Entity participating in any MIPS APM on any of the three snapshot dates (March 31, June 30, August 31), as well as December 31 during a performance period, would be considered participants in an APM Entity group. This would allow ACOs to capture all clinicians added to the ACO at any time in the performance year for purposes of determining the ACO final MIPS score and resulting payment adjustment.
MIPS Promoting Interoperability Changes
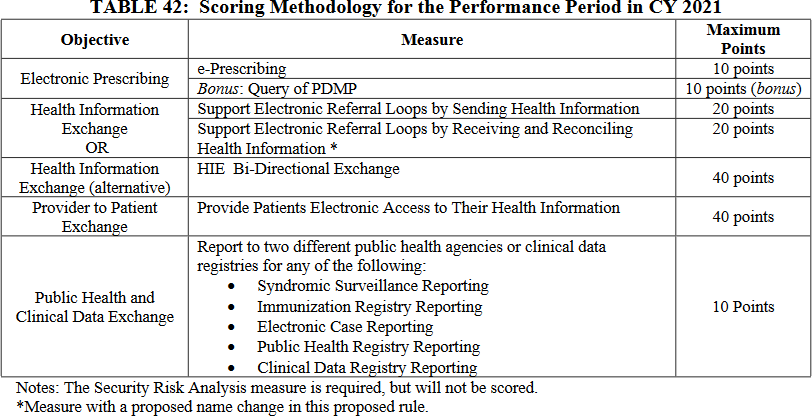
CMS proposes minimal changes to the scoring and measures used for the Promoting Interoperability performance category for 2021. These changes are outlined in Table 42 on page 50302.
CEHRT Changes Required by the 21st Century Cures ActCMS proposes to update the definitions of Certified EHR Technology (CEHRT) for the Promoting Interoperability Program and performance category of MIPS. CMS proposes that the technology must be certified to the current 2015 Edition certification criteria as specified in the 21st Century Cures Act.
MIPS Final Scoring and Projected MIPS Scores for 2021
CMS proposes that final scoring for APMs reporting through the APP would follow the same methodology currently established for the MIPS APM Scoring Standard. Specifically, CMS would continue to score each performance category and multiply each performance category score by the applicable performance category weight, and then calculate the sum of each weighted performance category score and apply any applicable adjustments to those appearing on the APM Participation List or Affiliated Practitioner List.
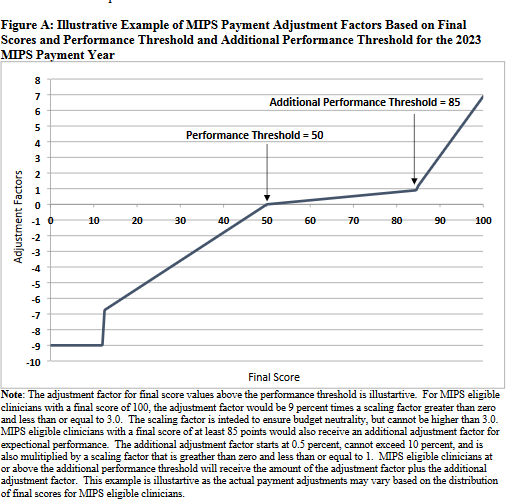
For 2021, CMS is proposing to reduce the generally applicable (non-ACO) MIPS performance threshold given challenges related to COVID-19. Given this change, CMS projects a lower maximum MIPS payment adjustment for PY 2021 corresponding to 2023 payments. CMS projects an approximately 7 percent payment adjustment in 2023 for those scoring 100 points in MIPS in PY 2021. More information on CMS’s projections are outlined in Figure A on page 50319 of the proposed rule.
Reweighting/Exceptions for COVID-19 for APM Entities Subject to MIPS
CMS proposes to allow an APM Entity to submit a hardship exception on behalf of all participants in the APM beginning with PY 2020. The request for reweighting would apply for all four MIPS performance categories and for all clinicians in the group subject to MIPS. If an APM Entity, such as an ACO, submits a hardship exception, CMS would not use any data submitted and the APM Entity would receive a neutral MIPS score and payment adjustment for the performance year. Additionally, APM Entities must demonstrate in their application to CMS that greater than 75 percent of its participant MIPS eligible clinicians would be eligible for reweighting the Promoting Interoperability performance category for the applicable performance period. As a reminder, MIPS hardship exceptions are due by December 31, 2020, for PY 2020 and may be submitted through the QPP website.
MIPS Quality Measure Updates for 2021
MIPS quality measures with proposed substantive changes can be found in Table Group D of Appendix one of the proposed rule. CMS proposes substantive changes to 112 MIPS quality measures.
Finally, note that CMS is also proposing to adjust the current MIPS quality measure benchmarking rules due to data anomalies presented by COVID-19. Specifically, CMS proposes to use CY 2021 data to determine PY 2021 quality benchmarks. Should CMS finalize these proposals, this will result in ACOs not knowing quality benchmarks in advance of the performance year. CMS seeks comment on alternative approaches.