The Impact of Retrospective Versus
Prospective Attribution on Your ACO
Background: Under changes made in the Pathways to Success regulations finalized in December 2018, Medicare Shared Savings Program (MSSP) ACOs can now choose between retrospective or prospective attribution in agreement periods starting in July 2019 and thereafter, and they can annually change this choice. Such changes can be made prior to the start of a performance period. This change was mandated by Congress through Section 50331 of the Bipartisan Budget Act passed in February 2018. Previously, ACOs in MSSP’s Track 1 and 2 could only use retrospective attribution, while ACOs in MSSP’s Track 3 and 1+ could only use prospective attribution. ACO models tested under the CMS Innovation Center, including the Next Generation ACO Model, Direct Contracting, and ACO REACH Model, only use prospective attribution. In 2022, 38 percent of MSSP ACOs use prospective attribution, compared to 62 percent that use retrospective attribution.
In both retrospective and prospective attribution, ACOs will experience changes over time in the beneficiaries for whom they are accountable. The methods used to identify the individual beneficiaries associated with an ACO are similar for each method, although the reasons for turnover or attrition during a performance year are often very different. In general, retrospective models reward ACOs that build and maintain strong beneficiary loyalty, while prospective models are often favored by ACOs that desire predictability and for whom retrospective attribution would disproportionately attribute patients new to the ACO because of aging into Medicare or from receiving ACO-based primary care because of hospital discharge. In 2018, NAACOS analyzed the differences in assigned population sizes and benchmarks yielded by selecting either attribution method.
NAACOS was supportive of CMS’s providing additional flexibility in ACOs’ choice of assignment and had previously called for CMS to make this allowance. Detailed information on the aspects of the different MSSP tracks is available in NAACOS’s ACO Comparison Chart. A separate NAACOS chart compares various high-risk ACO options, including MSSP Enhanced and ACO REACH.
Importance of Attribution: Attribution is a foundational aspect of ACO models and identifies individual patients for whom ACOs take accountability for. An ACO’s historical benchmark would be change based on attribution selection since the populations used to determine benchmark and performance year assignment would vary based on the ACO’s choice. Attribution also determines which beneficiaries are eligible for benefit enhancements such as telehealth visits and waivers of the requirement that patients have three-day inpatient hospital stay before a skilled nursing facility stay.
Attribution Definition: While MSSP refers to the methodology as “assignment” and the ACO REACH Model refers to it as “alignment,” this guide uses an all-inclusive term of “attribution” for consistency. In both MSSP and REACH, claims-based attribution is driven by analysis of utilization of primary care services. Primary care services are further defined as a specific set of qualified treatment codes, many of which are Evaluation and Management (E&M) codes. CMS uses more than 60 Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes for MSSP assignment and lists them in §425.400(c)(1).
Additional details on attribution are spelled out in MSSP regulations and the Participation Agreement of Global and Professional Direct Contracting, the precursor to ACO REACH. CMS also regularly updates guidance on financial and assignment specifications, which had its tenth version in 2022.
Overall Attribution Rules: CMS applies consistent approaches under both retrospective and prospective attribution:
- Beneficiaries who receive Medicare Advantage during the performance year are excluded from attribution.
- Beneficiaries who die during the performance year remain attributed.
- Beneficiaries have at least one month of Part A and Part B enrollment.
- Prospective overrides retrospective. A beneficiary prospectively attributed to an ACO will not be eligible for attribution to a different ACO, even if the beneficiary accumulates a plurality (the most primary care services charges, but not necessarily a majority) of primary care services from another ACO’s participants during a performance year.
- Place of residence impact:
- MSSP: CMS excludes beneficiaries whose permanent residence is outside of the United States or U.S. territories and possessions in the last month of the attribution window.
- ACO REACH: CMS excludes beneficiaries who reside outside of a county in the ACO’s service area.
- Accurate participant lists drive attribution:
- MSSP: CMS uses Tax Identification Numbers (TINs), and for Federally Qualified Health Centers (FQHCs) and Rural Health Centers (RHCs). CMS uses all possible National Provider Identifier (NPI) to CMS Certification Number (CCN) combinations.
- ACO REACH: CMS uses TIN to NPI combinations.
Explanation of Retrospective Attribution
Preliminary prospective assignment with retrospective reconciliation, as it is more formally called, uses a two-step process for assignment, as follows:
First step: A beneficiary is attributed to an ACO if the allowed charges for primary care services furnished to the beneficiary by primary care physicians (PCPs) who are ACO professionals and non-physician ACO professionals (i.e., physician assistant [PA], nurse practitioner [NP], and clinical nurse specialist [CNS]) in the ACO are greater than the allowed charges for primary care services furnished by PCPs and select non-physician professionals (i.e., PA, NP, and CNS), who are ACO professionals in another ACO or are not affiliated with any ACO.
Second step: (Only considers beneficiaries who have not had a primary care service rendered by any PCP, PA, NP or CNS inside or outside the ACO). The beneficiary will be attributed to an ACO if the allowed charges for primary care services furnished to the beneficiary by physicians, who are ACO professionals with specialty designations in §425.402(c), are greater than the allowed charges for primary care services furnished by physicians with specialty designations as specified §425.402(c), who are ACO professionals in any other ACO or who are unaffiliated with an ACO.
CMS preliminarily assigns beneficiaries at the beginning of a performance year based on most recent data available, and ACOs will receive an assignment list naming these preliminarily assigned beneficiaries. Assignment will be updated quarterly based on the most recent 12 months of data, and newly generated lists will be distributed to ACOs. For final assignment, the assignment window is the relevant 12-month calendar year.
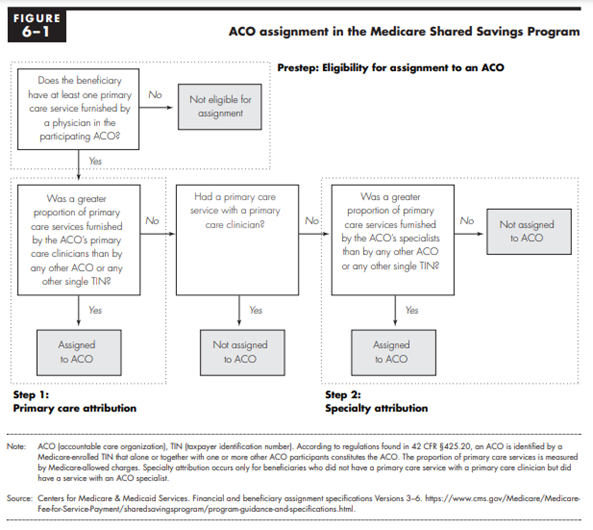
Source: Medicare Payment Advisory Commission June 2019 Report to Congress
Explanation of Prospective Attribution
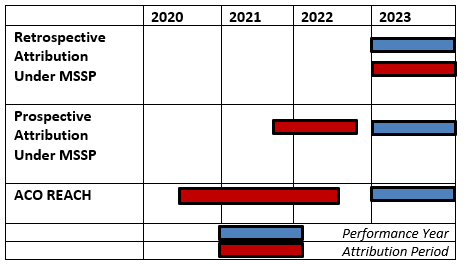
For these ACOs, CMS uses a process similar to that of retrospective assignment, which is based on where a beneficiary receives the plurality of primary care services. However, as illustrated in Figure 1 below, the timing of the assignment window is different, and this process results in a list of prospectively attributed beneficiaries. These beneficiaries are reflected in the data reports, quality reporting, and financial reconciliation for that ACO. Claims-based assignment is determined at the beginning of each benchmark and performance year based on the beneficiary’s use of primary care services in the most recent 12 months for which data are available. The prospective list is provided to the ACO close to the start of each performance year and cannot be increased.
Once a beneficiary is prospectively assigned to an ACO, the beneficiary is not eligible for assignment to a different ACO, even if they receive the plurality of their primary care in a different ACO during the relevant benchmark or performance year.
ACO REACH
Like with MSSP, CMS analyzes claims for beneficiaries who received care from an ACOs’ Participant Providers to determine the percentage of each beneficiary’s primary care services delivered by REACH providers in select primary care specialties or, for purposes of the second stage of the two-stage alignment algorithm, one of the select non-primary care specialists.
Beneficiaries will be aligned to an ACO if they receive the plurality of their qualifying primary care services from the ACO’s Participant Providers, either from primary care practitioners or select non-primary care specialists. If 10 percent or more of the allowable charges incurred for qualifying primary care services received by a beneficiary during the two-year alignment period are billed by physicians and practitioners with a primary care specialty, then alignment is based on the allowable charges incurred for services provided by primary care specialists. If it is less than 10 percent, then alignment is based on the allowable charges incurred for services provided by physicians and practitioners with certain non-primary specialties.
Figure 1: ACO Attribution Timeframes
Voluntary Alignment
CMS incorporates voluntary alignment into the attribution process for MSSP and ACO REACH. Through voluntary alignment, beneficiaries can identify their “primary clinician,” and, provided other criteria are met, such as receiving at least one primary care service during the assignment window from a physician in that ACO and the beneficiary designating an ACO professional in that ACO as his/her “primary clinician,” then the beneficiary will be attributed to that provider’s ACO, superseding any claims-based attribution. Designation is optional and done through MyMedicare.gov. Voluntary alignment first became an option for Performance Year 2018. More information on voluntary alignment is provided in this NAACOS resource.
The purpose of voluntary alignment is to encourage ACOs to work on establishing or confirming care relationships between ACO providers and beneficiaries. This allows ACOs to focus efforts and resources on segments of their beneficiary population that may not be aligned based on claims data but would benefit from a relationship with the ACO. It is important to note that voluntary beneficiary alignment does not obligate a beneficiary to receive care from a particular ACO, and the beneficiary still retains freedom to receive services from the Medicare provider of his/her choice.
CMS will also allow REACH ACOs to market to beneficiaries for purposes of voluntary alignment. REACH ACOs may proactively communicate with beneficiaries for the purpose of outreach regarding voluntary alignment. REACH ACOs may also elect to participate in Prospective Plus alignment, whereby beneficiaries that voluntarily align during a performance year will be added on a quarterly basis throughout the year. CMS will adjust the REACH ACO’s benchmark and capitated payments according. However, REACH ACOs should be aware that this option reduces the predictability of prospective benchmarks.
CMS also allows REACH ACOs to engage in “Paper-Based Voluntary Alignment,” which allows a beneficiary to voluntarily align to an ACO through a standard form provided by CMS. This process makes voluntary alignment much more accessible compared to MSSP because it allows REACH ACOs to have beneficiaries sign a form, rather than access MyMedicare.gov on their own.
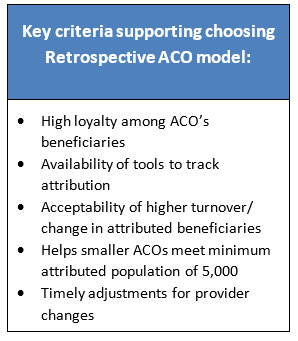
Pros and Cons of Retrospective Attribution:
Pros:
- Reduces potential inequalities in care by encouraging ACOs to redesign care for all patients. Without knowing which beneficiaries will ultimately be attributed, an ACO is more likely to implement processes to provide high quality and lower cost care to all patients equally. CMS cites this as a benefit for all Medicare beneficiaries.
- Enables smaller ACOs to participate. MSSP ACOs need to have at least 5,000 attributed beneficiaries to participate and remain in the program. Under retrospective attribution, ACOs can add beneficiaries throughout the year, which is helpful for ACOs near the 5,000-beneficiary threshold.
- Facilitates timely additions to the ACO. Beneficiary attribution may increase during the performance year when new beneficiaries begin to receive care from ACO participants.
- Recognizes additional providers joining the ACO. Providers who join the ACO during the performance year contribute to the calculation of plurality for potentially attributed beneficiaries.
- Favors ACOs with ability to track and follow-up on beneficiaries independently of CMS reporting. If an ACO can accurately monitor beneficiary use of primary care services during the performance year, the ACO can have very accurate predictions of which beneficiaries will ultimately be retrospectively attributed. Examples of events to track include beneficiaries eligible for annual wellness visits (AWVs) and those who receive primary care services from non-ACO participants. Therefore, ACOs adept at this tracking will know their final attributed beneficiaries well before CMS makes that information available to ACOs, which usually happens between May and August following the end of the performance year.
- Enables providers to focus on building long term relationships with beneficiaries. ACOs that implement programs to prevent attrition through appropriate preventive care and AWVs can build a loyal patient base.
Cons:
- Distracts ACOs with inaccurate information. There is usually significant turnover or “churn” in CMS’s quarterly reports of expected attributed beneficiaries. This churn is based on beneficiaries receiving primary care from multiple providers, some of whom are outside the ACO. It is not unusual for quarterly changes to be between 10 and 20 percent with some beneficiaries cycling in and out on alternating quarters. This can be particularly challenging for ACOs where this turnover is difficult to anticipate or track, which is often the case in rural and underserved areas.
- Diminishes patient-doctor relationships. An ACO may discover beneficiaries attributed for reasons that conflict with long-term patient-doctor relationships or goals of the ACO. For example, a beneficiary may have been a multi-year patient of a specific non-ACO participant, but if he or she is treated by an ACO participant the one time the beneficiary receives primary care services during a performance year, the beneficiary will be attributed to that ACO. Some ACOs are surprised when these beneficiaries are discovered during final reconciliation after the performance year.
- Penalizes ACOs with transplant programs. Some ACOs have experienced retrospective attribution of patients who have migrated into the ACO for transplant services, and as a result they have received a significant amount of primary care services before and after the transplant itself. These patients often experience higher costs during the transplant period than their risk adjustment might have predicted.
- Results in resource use that does not benefit the ACO. Because some ACOs cannot predict which beneficiaries will be attributed, an ACO may find itself utilizing its limited resources to intervene with a larger population of patients. While all those patients may benefit from services including care management, behavioral health, medication management, or post discharge planning, the ACO may later discover that these services were provided to beneficiaries attributed to another ACO or no ACO at all. While ACOs are committed to providing highly coordinated care for all patients, this can be a strain on the ACO’s resources.
- Beneficiary notifications. ACOs that use retrospective assignment are still required to send written beneficiary notifications to all fee-for-service (FFS) beneficiaries receiving primary care services from ACO providers. This can be costly and burdensome. Starting in 2022, ACOs that use prospective assignment will only be required to send notices to beneficiaries that have been prospectively assigned to their ACO.
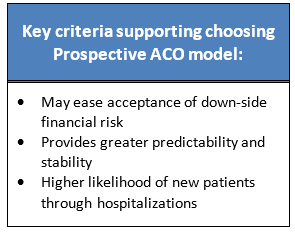
Pros and Cons of Prospective Attribution:
Pros:
- Allows ACOs to focus their population management resources. The resources, initiatives and processes to actively manage care for patients and engage beneficiaries are often a driver for lowering costs and allowing an ACO to earn shared savings.
- Gives providers stronger incentives to engage beneficiaries and their caregivers. Engaging just attributed beneficiaries and their caregivers in care management activities is easier with prospectively attributed beneficiaries and also enhances patient satisfaction, improves outcomes, and increases the probability the beneficiary will remain part of the ACO.
- Allows ACOs to establish stabilized financial targets. These targets are essential for an ACO to stay on track with managing costs throughout the performance year. Because the ACO knows no new beneficiaries will be added to panels during the performance year, establishing these targets is easier.
- Encourages transparency with attributed beneficiaries. Prospective attribution enables patients to be fully aware of any incentives providers may have in delivering their care and allows them to incorporate this understanding into their interactions with their care providers.
- Provides a timing benefit to an ACO. Prospective attribution reduces the potential quality measure and financial impact from beneficiaries who initiate receiving primary care services from an ACO’s participants during a performance year because those patients will not be attributed to the ACO until the subsequent performance year. In other words, if a beneficiary who has not previously received care from the ACO’s providers used in assignment presents at a hospital for admission and is subsequently provided primary care services by the ACO’s participants, that initial year’s experience will not be included in the ACO’s current performance year quality and financial measurement. Similar protections are provided for beneficiaries who age-in to Medicare during a performance year. Therefore, a forward-thinking ACO can ensure the beneficiary receives necessary care and appropriate diagnoses for risk adjustment in preparation for being added to prospective attribution in the subsequent performance year.
- Allows focused investment in ACO infrastructure. CMS notes that improved certainty under prospective attribution may be an important factor in an ACO’s willingness to take on greater performance-based risk because the ACO is better positioned to make decisions regarding where to make investments in infrastructure to deliver enhanced services because the population is known at the beginning of the performance year.
- Beneficiary notification. Starting in 2022, ACOs that use prospective assignment will only be required to send written beneficiary notifications to beneficiaries that have been prospectively assigned to their ACO. Meanwhile, ACOs that use retrospective assignment are still required to send notices to all fee-for-service (FFS) beneficiaries receiving primary care services from ACO providers. This relieves the ACO of a big cost and regulatory burden.
Cons:
- Maintains accountability even when the beneficiary receives care outside the ACO. ACOs are held accountable for prospectively attributed beneficiaries with whom their ACO participants have had little or no contact during the performance year and therefore have virtually no ability to effectively manage their care, quality, or costs.
- Can result in disparities of care processes for attributed versus non-attributed beneficiaries. Because some FFS Medicare beneficiaries presenting at ACO participants will not be part of the current year evaluation (i.e., the individuals not on the prospective listing), it is possible that discrimination or an appearance of disparity in application of time or resources could occur between identically insured patients based on attribution to the ACO.
- Diminishes patient-physician relationships. An ACO may discover beneficiaries attributed for reasons that conflict with long-term patient-doctor relationships. For example, a beneficiary may have been a multi-year patient of a specific non-ACO participant. But if during the attribution period the beneficiary happens to receive a plurality of primary care services from the ACO participants, the ACO will be attributed with the beneficiary. Some ACOs are surprised when these beneficiaries are on the prospective list, and accountability is established even though the beneficiary may never return to the ACO participants.
- Delays impact of changes in ACO providers. If providers join or depart from the ACO after submission of the provider list used for attribution and/or during the performance year, those changes are not reflected in the attributed patients until the next performance year.
Attribution Reporting: CMS provides Assignment Summary Reports with aggregate information on the ACO’s attributed beneficiaries including demographic and eligibility characteristics, proportion and number of primary care services provided to assigned beneficiaries, disease categories, and distribution of assigned beneficiary residence by county.
Retrospective Attribution: ACOs receive an initial assignment list of preliminarily prospectively attributed population near the start of each performance year, assignment lists for each benchmark year, quarterly reports on the ACO’s preliminary prospectively assigned population throughout each performance year, and a year-end report on retrospectively assigned beneficiaries used for financial reconciliation. These reports also identify beneficiaries that received a qualifying primary care service from an ACO participant during the year.
Prospective Attribution: ACOs receive a report of prospective attribution close to the start of each performance year, reports based on prospectively attributed beneficiaries for each benchmark year, quarterly reports based on the ACO’s currently attributed beneficiaries for the performance year that are updated to identify exclusions made in the year to date, and a year-end report on prospectively attributed beneficiaries for the performance year updated to identify beneficiaries no longer eligible for attribution at the end of the performance year.
Prospects for the Future: CMS periodically updates rules around attribution. In the 2022 Medicare Physician Fee Schedule, for example, CMS added seven more codes used in attribution. In 2021, CMS made other technical changes such as excluding advance care planning from being used to determine beneficiary assignment when billed in an inpatient setting. During the COVID-19 Public Health Emergency, CMS expanded the list of codes used in assignment to better account for the uptake of telehealth services, which was critical in the pandemic’s response.
The Medicare Payment Advisory Commission (MedPAC), which is an independent congressional agency that advises Congress on issues affecting Medicare payment to private health plans and providers, weighed in on attribution in its 2019 Report to Congress, following an examination of beneficiaries who regularly change ACO assignment and the use of AWVs. MedPAC suggested wider use, perhaps mandatory use, of prospective attribution to protect Medicare from ACOs seeking favorable patient selection through AWVs. That work is detailed in this NAACOS resource.
Moving forward, CMS could consider incorporating some attribution approaches found in commercial and Medicare Advantage contracts. For example, CMS could consider reconciling catastrophic expenses back to a previous ACO or provider for those that are incurred immediately following a beneficiary being attributed to a new ACO. This approach is used by some commercial payers especially where the episode is designated as preventable (e.g., certain readmissions, adverse events, hospital acquired conditions, or medical errors). Considering the significance of attribution, NAACOS continues to diligently monitor potential changes and comment to CMS about their immediate and long-term impact on ACOs.
Other Factors to Consider: ACOs deciding which attribution method to select or which ACO track to participate in can use the characteristics highlighted above to help them prioritize the attractiveness of tracks/models with retrospective versus prospective attribution. Additional factors to consider may include:
Beneficiary notification. Starting in 2022, ACOs that use prospective assignment are no longer required to send written beneficiary notifications to beneficiaries who have not been prospectively assigned to the ACO for the relevant performance year. Rather, ACOs will only be required to send notices to beneficiaries that have been prospectively assigned to their ACO. ACOs that use retrospective assignment are still required to send written notices to all FFS beneficiaries receiving primary care services from ACO providers. CMS made this change in the 2022 Medicare Physician Fee Schedule in order to eliminate potential confusion among beneficiaries receiving notices from ACOs to which they are not and will not be assigned.
Timing of attribution. There are differences between the MSSP and ACO REACH prospective attribution methods, especially with the timeframe of eligibility for and calculation of attribution. ACO REACH uses a 24-month period ending six months before the relevant performance year. MSSP bases prospective attribution on a 12-month window usually ending three months before the performance year. Retrospective assignment uses the calendar year that aligns with the performance year.
Providers used in attribution. ACO REACH uses a historical snapshot of providers submitted in June before the performance year. For prospective attribution in MSSP, attribution is based on the providers listed by the ACO, which are due in late summer or early fall. MSSP’s retrospective attribution is based on providers in ACO-participant TINs who furnish care to beneficiaries during the performance year. In both MSSP and ACO REACH, primary care physicians are the central focus for attribution, but certain specialty physicians and non-physician practitioners also play a role.
Prospective attribution attrition is front loaded. The exclusion of a majority of beneficiaries initially attributed under prospective assignment who will occur during the first quarter due to Medicare Advantage enrollment. These exclusions are usually communicated by CMS by late April or May of the performance year. While similar Medicare Advantage related attrition occurs to retrospectively attributed ACOs because beneficiaries are added and excluded at a significant pace throughout the performance year, attrition is more evenly distributed for retrospectively attributed ACOs.
Commercial ACO Contract Attribution Methodologies
ACOs report many variations on the retrospective and prospective attribution models used by commercial payers. Many commercial, Medicare Advantage, and managed care Medicaid contracts enforce prospective attribution by naming a specific primary care provider or practice for each covered person. Some contracts use default or assignment of a primary care provider when the covered person does not or cannot designate one. This approach helps establish a specific provider or practice as the initial building block for attribution. While no ACO touted its contracts as perfect, most ACOs reported that they value improved stability and predictability to help them achieve improved quality, cost, and patient as well as physician satisfaction.
Some contracts use retrospective attribution based on covered person behavior within the network associated with the contract. According to ACO feedback for this resource, the least popular method was based on using the most recent primary care visit to associate a covered person with an ACO. ACOs also reported that frequency or volume of primary care was commonly used to drive retrospective attribution. In general, these retrospective attribution approaches may not be as popular as prospective with the provider community but are convenient for payers because of the “end of period” accuracy.
Commercial and Medicare Advantage contracts are often the product of negotiation and therefore reflect the variety of leverage providers and payers bring to the table. As ACOs enter into or revise contracts with commercial payers, it is important to negotiate an attribution methodology that is beneficial to the ACO.
References:
§425.400 Subpart E—Assignment of Beneficiaries
Pathways to Success Final Rule – December 2018
NAACOS Analysis of the Final MSSP Pathways to Success Rule
NAACOS’s Evaluation of Potential ACO Performance Bias from Retrospective and Prospective Assignment – June 2018
MSSP’s Shared Savings and Losses and Assignment Methodology – Version 9
GPDC Performance Period 1 Participation Agreement
ACO REACH Request for Applications
June 2019 MedPAC Report to Congress on MSSP assignment methodology