ACO REACH Model Performance Year 2024 Model Updates
On August 14, 2024, CMS’s Center for Medicare and Medicaid Innovation (the Innovation Center) released a document describing, at a high level, changes it will be implementing to the ACO REACH Model for Performance Year 2024. The Innovation Center will provide additional details on these changes in a series of policy papers that it expects to release later this year. It will formalize the new policies through an amendment to the Participation Agreement prior to the start of 2024.
NAACOS appreciates that CMS continues to improve on the ACO REACH Model by addressing many concerns raised by NAACOS members. These include financial protections from midyear changes to benchmarks, additions to the Health Equity Benchmark Adjustment to account for more patient characteristics, and updates to its risk adjustment policies. We believe these changes will satisfy many concerns and stabilize future participation and will continue to advocate for additional changes, including further revisions to the model’s benchmarking methodology. Additionally, we encourage CMS to explore adding features of REACH into a permanent track within the Medicare Shared Savings Program (MSSP). Using MSSP as a chassis for innovation while infusing lessons learned from Innovation Center models into a permanent program is another path for stabilizing and growing participation in ACOs.
Beneficiary Alignment
Reduction in alignment minimums for New Entrant and High Needs ACOs
New Entrant ACOs: The Innovation Center is reducing the minimum number of aligned beneficiaries for 2025 from 5,000 to 4,000. New Entrant ACOs will still only need 3,000 beneficiaries for 2024 and will need 5,000 aligned beneficiaries for 2026.
High Needs ACOs: The Innovation Center is reducing the minimum number of aligned beneficiaries for PY2025 (from 1,200 1,000) and PY2026 (from 1,400 to 1,250). For PY2024, High Needs ACO will still need only 750 beneficiaries.
|
New Entrant ACOs |
High Needs ACOs |
|||
|
Performance |
Previous Minimums |
New Minimums |
Previous Minimums |
New Minimums |
|
2024 |
3,000 |
3,000 |
750 |
750 |
|
2025 |
5,000 |
4,000 |
1,200 |
1,000 |
|
2026 |
5,000 |
5,000 |
1,400 |
1,250 |
Protection again fluctuating alignment numbers
Beginning in 2024, the Innovation Center is implementing a “buffer” against drops in beneficiary alignment for all REACH ACOs. ACO alignment may temporarily drop below the required minimum by up to ten percent (10 percent) in a performance year. The Innovation Center will apply the buffer policy only one time across the remaining three performance years. ACOs do not need to request application of the buffer, as the Innovation
Center will automatically apply it if it determines an ACO has fallen below the alignment minimum.
Additional eligibility criteria for High Needs ACOs
The Innovation Center is expanding the beneficiary pool eligible for alignment to a High Needs ACO.
Current Criteria: Beneficiaries with one or more conditions that impair mobility or neurological condition, significant chronic or other serious illness reflected by risk score and unplanned hospital admissions, or signs of frailty.
New Expanded Criteria: Beneficiaries with at least 90 Medicare-covered days of Home Health services utilization or at least 45 Medicare-covered days in a Skilled Nursing Facility within the previous 12 months.
NAACOS appreciates the Innovation Center’s desire to appropriately capture patients that would benefit from highly coordinated care under a High Needs ACO. However, we are monitoring the change to ensure it does not pull beneficiaries away from Standard ACOs and we continue to believe that ACOs should be able to participate in multiple tracks of the ACO REACH Model.
Financial Guarantees
Change to “stacking” policy
Currently ACOs must keep their financial guarantee for a given performance year in place until Final Settlement for the PY. Under the new policy, ACOs participating in Provisional Financial Settlement may release the required financial guarantee amount for a performance year after they have fully paid any Shared Losses reflected in the Provisional Financial Settlement report. In other words, an ACO would not have to “stack” financial guarantees. This change will reduce by about six months the amount of time an ACO must carry the costs of the financial guarantee for a performance year.
Increased financial guarantee for Enhanced Primary Care Capitation and the Advanced Payment Option (APO)
Beginning in 2024, CMS is increasing the financial guarantee amount for all ACOs participating in Enhanced Primary Care Capitation and the APO.
|
|
Current amount |
New amount |
|
Professional Risk ACOs |
2.5 percent |
4 percent |
|
Global Risk ACO |
3 percent |
4 percent |
Historically, ACOs could reduce the costs to participate in the model by electing to participate as Professional Risk ACOs. NAACOS is concerned that this change further increases the operating costs incurred by ACOs to participate in the model and will put a strain on continued participation. While the Innovation Center states the change is necessary to mitigate risk associated with changes in settlement numbers between Provisional Financial Settlement and Final Settlement, NAACOS believes that the change in calculation of Provisional Settlement (see below) already addresses that concern and that any additional financial risk should be borne by CMS.
Provisional Settlement
Expansion of experience period
Currently, Provisional Settlement reflects only six months of a given performance year, with another six months of run-out. Under the change, beginning in 2024, the Innovation Center will use a full 12 months of performance year experience. In addition to providing improved accuracy to the Provisional Settlement, the change means the Provisional Settlement report should align with the fourth quarter Quarterly Benchmark Report for a performance year.
NAACOS supports this policy change. We will also advocate for the Innovation Center to extend this policy to PY2023 (for settlement taking place in calendar year 2024).
Benchmarking
Revisions to the Health Equity Benchmark Adjustment (HEBA)
Underserved beneficiary qualifications: The Innovation Center currently uses a blend of the Area Deprivation Index (API) and dual Medicare-Medicaid eligibility to determine which beneficiaries qualify for the upward and downward HEBA. The Innovation Center has stated historically that it would seek to revise these qualifications to better capture underserved beneficiaries. Under the new policy, the Innovation Center is adding two additional components: Low-Income Subsidy Status (in combination with dual eligibility as a single component) and the state-based ADI. The three components will be weighted equally.
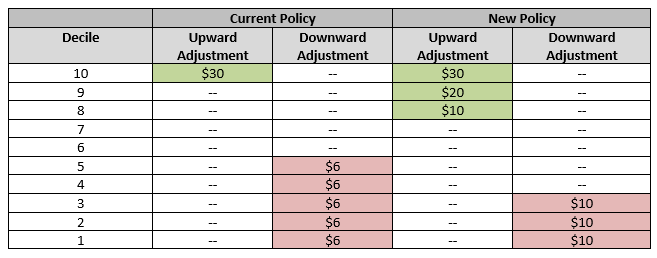
Application of HEBA deciles: Beginning in 2024, the Innovation Center will expand the upward adjustment while narrowing the downward adjustment.
Addition of Retrospective Trend Adjustment (RTA) risk corridors
Under current policy, the Innovation Center may adjust the RTA if the actual trend varies from the prospective trend by at least 1 percent. Beginning in 2024, the Innovation Center will apply risk corridors to changes between RTA and actual trend to offer some predictability and protection to ACOs.
|
% Change (positive or negative) between RTA and actual trend |
Financial Responsibility for Change |
|
|
|
ACO |
CMS |
|
Up to 4 percent |
100 percent |
0 percent |
|
4-8 percent |
50 percent |
50 percent |
|
>8 percent |
0 percent |
100 percent |
NAACOs appreciates the Innovation Center’s efforts to address this issue but believes too much financial responsibility remains with ACOs. Changes to the RTA have a significant impact on the viability of model participation for ACOs, and a 4 percent upward adjustment can be financially devasting to ACOs. CMS should take more responsibility for its own trend calculations, and NAACOS will advocate for a revision to the risk corridors accordingly.
Application of 2024 new risk adjustment model
Earlier this year, CMS announced the new risk adjustment model in 2024, an update of the 2020 risk adjustment model. For 2024, the Innovation Center will blend the 2024 and 2020 models, weighting the new 2024 at 67 percent and the 2020 model at 33 percent. The same blend will be applied to both baseline years and performance years. The Innovation Center expects the change to reduce ACO benchmarks by -0.4 percent.
NAACOS supports the Innovation’s Center’s desire to decrease the impact of the new risk adjustment model on ACO benchmarks. We will work with the Innovation Center in reevaluating the blend of models in future model years to minimize the impact over the duration of the model.
Confirmation of static risk score growth reference year
As previously announced, beginning in 2024, the Innovation Center will move to a static reference year with a demographic adjustment in calculating the risk score growth cap for Standard and New Entrant ACOs. Under the static reference year policy, ACOs will be subject to a +/-3 percent cap on risk score growth across the remaining three model years. In other words, an ACO’s risk score will no longer be able to grow by 3 percent each performance year and can only grow by up to 3 percent total for the duration of the model.
NAACOS does not support this policy change, which will serve as a hindrance to CMS’s stated goal of improving health equity through care to underserved beneficiaries. We fear that continuing with the policy will make the model financial unsustainable for many ACOs. NAACOS also supports a future change to remove underserved beneficiaries (e.g. the top three deciles) from the cap calculation during their first year of alignment. Further, we understand that the Innovation Center is working on significant revisions to the model’s financial methodology for 2025 and 2026 and will advocate for revisions that ensure the model remains a viable option for ACOs.
Cap on Coding Intensity Factor (CIF)
Under current policy, there is no cap on the CIF applied to ACO risk score growth. Beginning in 2024, the Innovation Center will apply a 1 percent cap on the CIF, which will limit exposure of the adjustment to ACOs.
NAACOS supports this change. We are analyzing the true financial impact of the change in conjunction with the static reference year. NAACOS also appreciates that the change will limit the impact of high risk score ACOs (those that focus on full and completed coding) on those that do not have a similarly focus on beneficiary coding.
Application of risk adjustment to High Needs ACOs
Beginning in 2024, the Innovation Center will apply the +/-3 percent risk score cap policy and CIF to High Needs ACOs. High Needs ACOs will continue to use the CMMI-HCC concurrent risk adjustment model.
NAACOS believes that ACOs must be able to accurately reflect the risk of their aligned beneficiary population and is especially concerned about the impact of the cap and CIF on the vulnerable and less predictable high needs population. We also believe that the Innovation Center should apply the concurrent risk adjustment model to “high needs” beneficiaries in all REACH ACOs.
Benefit Enhancements
Expansion of the Nurse Practitioner (NP) and Physician Assistant (PA) Services Benefit Enhancement
Beginning in 2024, NPs and PAs that are Participant Providers or Preferred Providers with a REACH ACO participating in the NP/PA Benefit Enhancement will be able to certify and order Pulmonary Rehabilitation Care Plans.
NAACOS supports this expansion of the Benefit Enhancement.